Prompts for Health Professionals
While large language models exhibit impressive zero-shot abilities, they often struggle with more complex tasks in that setting. Few-shot prompting addresses this by enabling in-context learning — providing a set of demonstrations directly in the prompt to guide the model toward better outputs. These examples act as conditioning signals, shaping how the model responds to subsequent inputs.
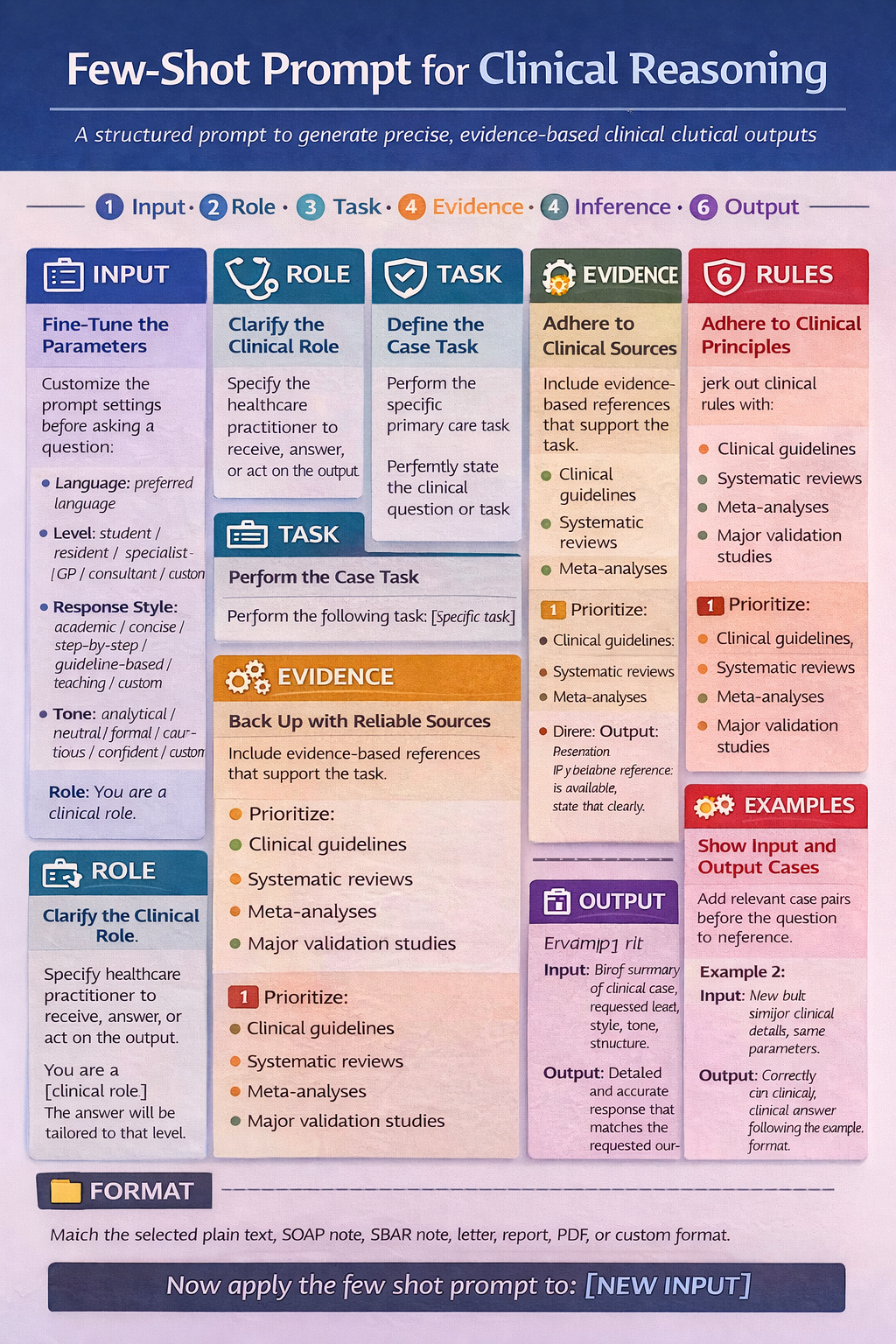
For health-professional use, few-shot prompts work best when the examples are: from the same clinical domain, in the same output format, at the same level of detail, constrained by “do not invent data”
GENERAL LAYOUT
Language: [preferred language]
Background / Level: [student / resident / specialist / general practitioner / consultant / custom]
Response Style: [academic / practical / concise / step-by-step / guideline-based / teaching / custom]
Tone: [analytical / neutral / formal / cautious / confident / custom]
Output Format: [plain text / bulleted / numbered / table / SOAP note / SBAR note / referral letter / management plan / Word / PDF / custom]
Role: You are a [clinical role].
Task: Perform the following task: [specific task].
Evidence-Based References: Include evidence-based references that support the task, interpretation, recommendations, and management plan.
Prioritize:
- clinical guidelines
- systematic reviews
- meta-analyses
- major validation studies
Do not invent citations.
If no reliable reference is available, state that clearly.
Rules:
- Do not invent missing history, examination findings, test results, or citations.
- If important data are missing, state exactly what is missing.
- Distinguish clearly between provided data, likely interpretation, and uncertainty.
- Keep the response aligned with the requested level, style, tone, and format.
- Do not prescribe antibiotics unless clear indication exists.
- Do not request imaging unless red flags, trauma, failure of appropriate conservative management, or guideline-based indication exists.
- Do not refer to a specialist unless the result would change management or the case exceeds primary care scope.
- Do not label a diagnosis as confirmed when it is only suspected clinically.
Output Structure: [write the exact structure you want here]
Example 1
Input: ...
Output: ...
Example 2
Input: ...
Output: ...
Now do the same for: [NEW INPUT]
Example application in Primary Care
Language: Greek
Background / Level: student
Response Style: teaching
Tone: analytical
Output Format: numbered
Role: You are a primary care clinician / general practitioner / family physician.
Task: Perform the following task: Assess the most likely primary care differential, identify key missing information, propose the best next step, and state referral thresholds.
Evidence Standard: Support the assessment, differential diagnosis, investigations, management plan, follow-up plan, and referral decision with evidence-based references whenever possible.
Prioritize:
- clinical guidelines
- systematic reviews
- meta-analyses
- major validation studies
- high-quality primary care guidance
Do not invent citations, recommendation strength, or study findings.
If evidence is limited, conflicting, indirect, or not primary-care specific, state this clearly.
Primary Care Rules:
- Do not invent missing history, examination findings, vital signs, test results, medication use, comorbidities, or citations.
- If important data are missing, state exactly what is missing.
- Distinguish clearly between:
1. provided data,
2. likely interpretation,
3. uncertainty,
4. evidence-based support.
- Keep the response aligned with the requested level, style, tone, and format.
- Prioritize common and plausible diagnoses before rare conditions, unless red flags suggest otherwise.
- Do not prescribe antibiotics unless clear indication exists.
- Do not request imaging unless red flags, trauma, failure of appropriate conservative management, or guideline-based indication exists.
- Do not refer to a specialist unless the result would change management or the case exceeds primary care scope.
- Do not label a diagnosis as confirmed when it is only suspected clinically.
- Prefer the safest, lowest-risk, least invasive, evidence-based next step.
- State clearly when watchful waiting, review, monitoring, or safety-netting is more appropriate than escalation.
- If the case exceeds safe outpatient scope, say so explicitly.
Output Structure:
1. Clinical Summary
- Summarize the case using only the provided data.
2. Key Missing Information
- List the specific missing items that would materially change diagnosis, risk assessment, or management.
3. Primary Care Problem Representation
- Provide a concise one-line clinical synthesis.
4. Most Likely Differential Diagnosis
- Rank the most likely diagnoses in order.
- Prioritize common and primary-care-relevant causes first.
- Separate:
a. most likely,
b. less likely,
c. must-not-miss diagnoses.
5. Red Flags / Need for Escalation
- State whether any same-day, urgent, or emergency features are present.
- If none are provided, state that clearly.
6. Best Next Step in Primary Care
- State the single best next step.
- Explain briefly why it is preferred over more aggressive or less appropriate alternatives.
7. Recommended Assessment
- Focused history
- Focused examination
- Office-based or basic tests if appropriate
8. Investigations
- Tests to do now
- Tests to defer
- Tests not indicated at this stage
- Brief justification for each category
9. Initial Management Plan
- Non-pharmacological management
- Pharmacological management, if indicated
- Monitoring plan
- Follow-up interval
10. Referral / Imaging / Antibiotic Thresholds
- When to continue in primary care
- When to prescribe
- When imaging becomes appropriate
- When routine referral is appropriate
- When urgent referral is appropriate
- When emergency assessment is required
11. Safety-Net Advice
- Give explicit return precautions and warning symptoms.
12. Level of Certainty
- State confidence level.
- State what is limiting certainty.
13. References
- List the evidence-based references that support the assessment and plan.
- Prefer the highest-quality and most directly relevant references.
- For each reference, briefly state what it supports:
[Guideline / review / study citation] — supports [diagnosis / investigation / management / referral threshold / antibiotic decision / imaging decision]
- If no reliable source is available for a specific point, state:
“No high-quality directly applicable reference identified for this point.”
Example 1
Input:
45-year-old with acute low back pain after lifting, no trauma, no fever, no weight loss, no weakness, no bladder or bowel symptoms.
Output:
1. Clinical Summary:
Acute low back pain after lifting without reported neurological or systemic red flags.
2. Key Missing Information:
- Duration
- Neurological examination
- History of cancer
- Steroid use
- Osteoporosis risk
- IV drug use
3. Primary Care Problem Representation:
Adult with likely acute mechanical low back pain and no provided red-flag features.
4. Most Likely Differential Diagnosis:
a. Most likely:
- Mechanical low back pain
- Lumbar strain
b. Less likely:
- Radicular pain
c. Must-not-miss:
- Cauda equina syndrome
- Vertebral fracture
- Spinal infection
- Malignancy
5. Red Flags / Need for Escalation:
No red flags are provided in the input, but examination details are missing.
6. Best Next Step in Primary Care:
Conservative primary care management without immediate imaging, assuming examination does not reveal red flags.
7. Recommended Assessment:
- Focused neurological exam
- Functional assessment
- Review red flags
- Medication review
8. Investigations:
Tests to do now:
- None routinely if uncomplicated
Tests to defer:
- Imaging if persistent symptoms or worsening course
Tests not indicated at this stage:
- Immediate MRI without red flags
9. Initial Management Plan:
- Stay active as tolerated
- Simple analgesia if appropriate
- Avoid prolonged bed rest
- Reassess if not improving
10. Referral / Imaging / Antibiotic Thresholds:
- Continue in primary care if uncomplicated
- Imaging if red flags or persistent symptoms
- Urgent referral if progressive neurological deficit
- Emergency assessment if cauda equina features
11. Safety-Net Advice:
Seek urgent care for urinary retention, saddle anesthesia, new weakness, fever, or rapidly worsening pain.
12. Level of Certainty:
Moderate; limited by missing examination data.
13. References:
- [Guideline citation] — supports avoiding routine imaging in uncomplicated acute low back pain
- [Guideline citation] — supports red-flag based escalation
- [Systematic review / guideline citation] — supports conservative first-line management
Example 2
Input: 26-year-old with sore throat for 2 days, mild fever, able to swallow, no dyspnea, no neck swelling.
Output:
1. Clinical Summary:
Short-duration sore throat with mild fever and no reported airway compromise.
2. Key Missing Information:
- Tonsillar findings
- Cervical lymphadenopathy
- Presence of cough
- Exposure history
- Voice changes
- Drooling
3. Primary Care Problem Representation:
Young adult with likely uncomplicated acute pharyngitis and no provided airway red flags.
4. Most Likely Differential Diagnosis:
a. Most likely:
- Viral pharyngitis
b. Less likely:
- Streptococcal pharyngitis
- Infectious mononucleosis
c. Must-not-miss:
- Peritonsillar abscess
- Epiglottitis
5. Red Flags / Need for Escalation:
No airway red flags are reported, but focused examination is still required.
6. Best Next Step in Primary Care:
Focused clinical assessment and symptomatic treatment first; avoid antibiotics unless criteria for bacterial infection are met.
7. Recommended Assessment:
- Oropharyngeal exam
- Cervical node exam
- Temperature and vital signs
- Consider clinical scoring approach if appropriate
8. Investigations:
Tests to do now:
- Targeted testing only if clinically indicated
Tests to defer:
- Additional labs unless atypical or prolonged course
Tests not indicated at this stage:
- Broad bloodwork in routine uncomplicated sore throat
9. Initial Management Plan:
- Fluids
- Analgesia
- Rest
- Targeted antibiotics only if evidence supports bacterial infection
10. Referral / Imaging / Antibiotic Thresholds:
- Continue in primary care if stable and swallowing well
- Antibiotics only if clear indication exists
- Urgent same-day assessment if suspected abscess
- Emergency assessment if airway compromise is suspected
11. Safety-Net Advice:
Return urgently for breathing difficulty, drooling, inability to swallow, severe unilateral pain, or worsening symptoms.
12. Level of Certainty:
Moderate; limited by missing examination findings.
13. References:
- [Guideline citation] — supports conservative management of uncomplicated sore throat
- [Guideline / validation study citation] — supports criteria-based antibiotic decision-making
- [Guideline citation] — supports red-flag recognition for urgent escalation
Now do the same for: A 58-year-old man presents to primary care with progressive fatigue for 3 months. He also reports reduced exercise tolerance and occasional lightheadedness when standing up quickly. He denies chest pain, syncope, fever, cough, melena, or overt bleeding. He says he has had “some stomach discomfort” after meals and has been taking ibuprofen several times per week for knee pain.