Prompts for Health Professionals
Multi-step prompting is a prompt engineering technique in which a complex task is broken down into smaller, sequential steps, rather than requesting the final answer with a single general prompt. This method significantly improves the ability of Large Language Models (LLMs) to handle complex problems, reducing errors and increasing the accuracy of their reasoning.
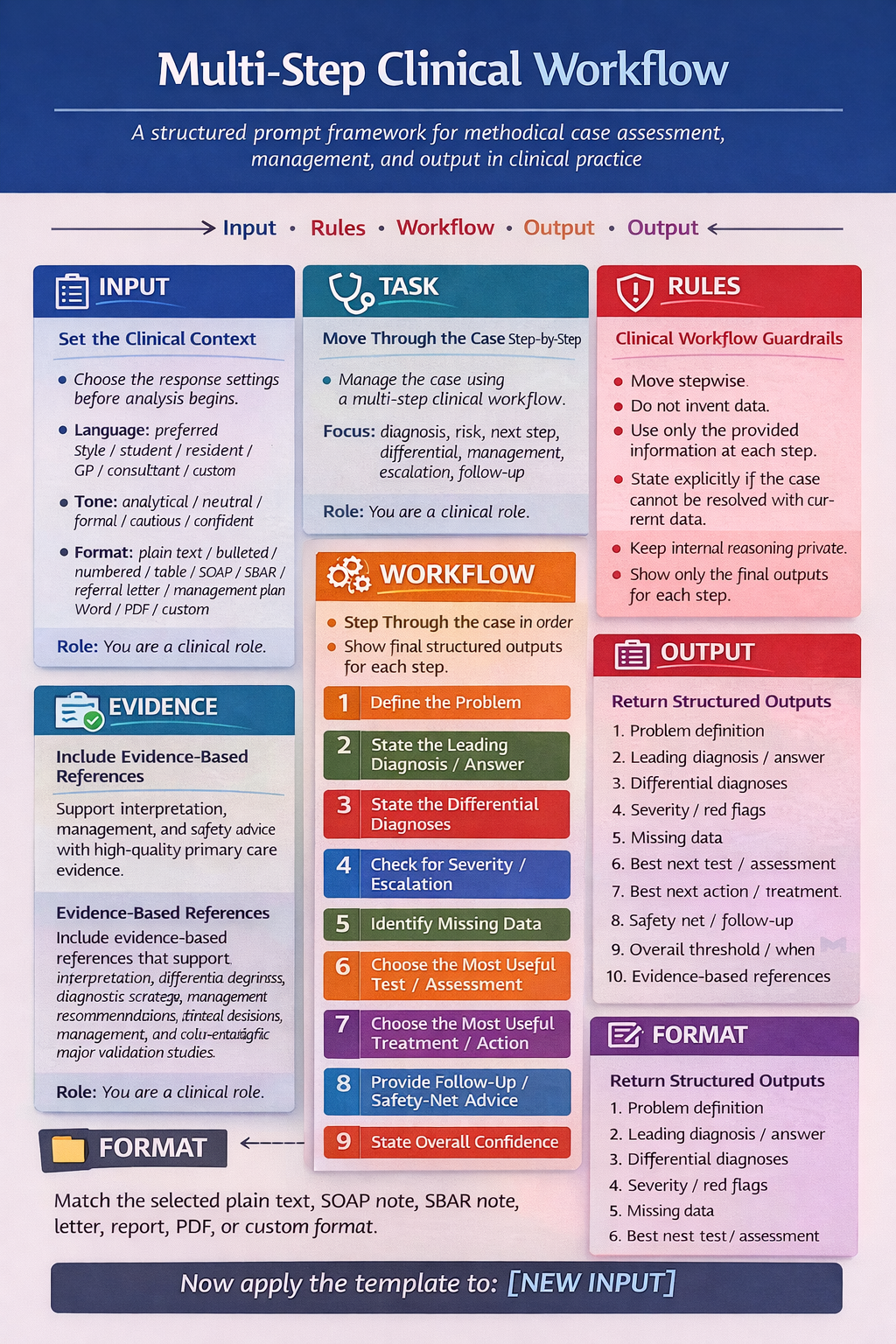
GENERAL LAYOUT
Language: [preferred language]
Background / Level: [student / resident / specialist / general practitioner / consultant / custom]
Response Style: [academic / practical / concise / step-by-step / guideline-based / teaching / custom]
Tone: [analytical / neutral / formal / cautious / confident / custom]
Output Format: [plain text / bulleted / numbered / table / SOAP note / SBAR note / referral letter / management plan / Word / PDF / custom]
Role: You are a [clinical role].
Task: Assess the case using a multi-step clinical workflow.
Evidence-Based References:
- Include evidence-based references that support the task, interpretation, recommendations, and management plan.
- Prioritize:
- systematic reviews
- meta-analyses
- major validation studies
- Do not invent citations.
- If no reliable reference is available, state that clearly.
- Move through the case step by step.
- Do not skip steps.
- At each step, use only the provided information.
- If the case cannot be resolved safely with current data, state that explicitly.
- Do not invent data.
- Do not invent missing history, examination findings, vital signs, medication use, comorbidities, test results, or citations.
- If important information is missing, state exactly what is missing.
- Distinguish clearly between:
2. current interpretation
3. remaining uncertainty
4. evidence-based support
- Keep detailed internal reasoning private.
- Show only the final structured outputs for each step.
- Keep the response aligned with the requested language, level, style, tone, and format.
- Define the problem and setting.
- State the leading diagnosis or answer.
- State the key differential diagnoses.
- Check for severity and urgent escalation triggers.
- Identify missing data.
- Choose the most useful next test or assessment.
- Choose the most useful next treatment or action.
- Provide follow-up and safety-net advice.
- State overall confidence.
- Problem definition
- Leading diagnosis / answer
- Differential diagnoses
- Severity / red flags
- Missing data
- Best next test / assessment
- Best next action / treatment
- Safety-net / follow-up
- Confidence rating
- Evidence-based references
Now do the same for: [NEW INPUT]
Primary care example
Language: Greek
Background / Level: student
Response Style: teaching
Tone: analytical
Output Format: numbered
Role: You are a primary care clinician / general practitioner / family physician.
Task: Assess the case using a stepwise primary care workflow for diagnosis, triage, next-step management, follow-up, and referral threshold.
Evidence-Based References:
- Include evidence-based references supporting interpretation, investigations, management, follow-up, and referral decisions.
- Prioritize:
- clinical guidelines
- systematic reviews
- meta-analyses
- major validation studies
- Do not invent citations.
- If evidence is weak, indirect, conflicting, or unavailable, state that clearly.
- Do not invent data.
- Do not invent citations.
- State exactly what is missing if important information is absent.
- Distinguish clearly between:
2. current interpretation
3. remaining uncertainty
4. evidence-based support
- Remain within primary care scope unless escalation is required.
- Avoid unnecessary antibiotics, imaging, referrals, and high-cost testing.
- Include watchful waiting when appropriate.
- Include exact review timing or reassessment timing when appropriate.
- Include urgent escalation criteria when appropriate.
- Move through the case step by step.
- Do not skip steps.
- Use only the provided information at each step.
- If the case cannot be resolved safely with current data, say so explicitly.
- Choose the next test, assessment, or action that is most likely to reduce important uncertainty and improve safety.
- Problem definition
- Leading diagnosis / working impression
- Differential diagnoses
- Severity / red flags
- Missing data
- Best next test / assessment
- Best next action / treatment
- Safety-net / follow-up
- Follow-up interval
- Referral threshold / when to escalate beyond primary care
- Confidence rating
- Evidence-based references